A physician managing a busy emergency department shift sees an average of 30 to 40 patients. In the same hours, the global medical literature grows by thousands of new papers. No clinician, however experienced, can absorb that volume in real time. That gap between what a clinician knows and what the full evidence base contains is not a training failure; it is a structural constraint, and artificial intelligence (AI) in clinical decision making is one of the most credible tools we have to close it.
The AI-powered clinical decision support system (CDSS) market was valued at $3.02 billion in 2025 and is projected to reach $18.28 billion by 2035. 71% of U.S. acute-care hospitals have already integrated predictive AI into their electronic health record (EHR) systems. The question is no longer whether to adopt AI in clinical decision making. It is whether to deploy it in a way that genuinely improves decisions, or one that creates a new layer of noise.
Key takeaways
- You will understand how AI-based CDSS works in practice and where it is delivering measurable clinical outcomes.
- You will see where AI predictive analytics in healthcare is producing hard evidence, from sepsis detection to readmission reduction.
- You will learn what AI in remote patient monitoring enables beyond hospital walls, and why the market is growing at 27% annually.
- You will get an honest account of the real barriers: explainability, bias, EHR integration, and alert fatigue.
- You will understand what responsible deployment of an AI clinical decision support system looks like, and why the interface layer matters as much as the model.
What AI in clinical decision making actually means
AI in clinical decision making refers to the use of machine learning (ML), natural language processing (NLP), and generative AI to support clinicians in diagnosing conditions, selecting treatments, predicting deterioration, and managing care pathways. It does not replace clinical judgment; it gives that judgment more accurate, more complete information to work with, faster.
The core mechanism is the CDSS: software that analyses patient data from EHRs, lab results, imaging, vital signs, and clinical notes, then surfaces risk scores, alerts, or treatment recommendations at the point of care. Early CDSS were rule-based systems that flagged drug interactions or prompted protocol steps. Modern AI-based CDSS are different in kind. They identify patterns across patient populations simultaneously, draw on real-time data, and generate probabilistic risk assessments no rule-based system could produce.
That matters because a significant proportion of clinical decision errors stem not from incompetence but from cognitive overload: too much information, too little time, and the anchoring biases that affect any human reasoning under pressure. The Stanford–Harvard State of Clinical AI report (2025) identified clinical decision support as one of the most active research areas in the field precisely because the structural problem is so large.
How AI-powered diagnostics are reducing errors across specialties
AI-powered diagnostics reduce clinical errors by processing imaging, pathology, and patient history at a consistency that human cognition cannot sustain across a full shift.
- AI-supported hospitals reported a 42% reduction in diagnostic errors compared to non-AI facilities.
- A prospective multicentre study (2025) found radiologists working with AI achieved 98.91% sensitivity in detecting intracranial haemorrhage versus 95.91% for standalone AI. That 3-percentage-point gap translates directly into missed diagnoses at scale.
- In gastroenterology, AI image recognition identifies polyps during colonoscopy review, freeing endoscopists for ambiguous or high-complexity cases.
- In pathology, AI-assisted tissue analysis accelerates biopsy slide triage.
- For rare diseases, AI trained on diverse datasets surfaces similar historical cases and narrows differential diagnoses in timeframes that manual research cannot match.
There is an important caveat. The Stanford–Harvard report documented cases where clinicians followed incorrect AI recommendations even when errors were detectable, producing worse outcomes than without AI input. The implication is clear: training clinicians to interrogate AI outputs critically is as important as the accuracy of the model itself.
AI predictive analytics in healthcare: moving from reactive to preventive care
AI predictive analytics in healthcare identifies deterioration, disease progression, and adverse events before they become critical, shifting care from reactive to proactive. The numbers are specific:
- Organisations using AI predictive analytics report 32% better sepsis detection and 20% fewer readmissions versus standard monitoring.
- One health system using AI-guided remote monitoring cut 30-day readmissions by 70% and reduced cost of care by 38%.
- In April 2024, the FDA authorised the Sepsis ImmunoScore, the first AI-based diagnostic tool for sepsis prediction, incorporating 22 parameters from demographics, vital signs, and lab tests to flag at-risk patients within 24 hours.
When a predictive model flags a deteriorating patient early, clinical teams can adjust acuity, prioritise interventions, and initiate care pathways before a crisis develops. A clinician using AI-informed risk stratification focuses diagnostic attention where it is most likely to change the care decision, reducing unnecessary tests and compressing time-to-diagnosis. At a population level, AI predictive analytics helps hospital systems identify under-screened cohorts, recurring care gaps, and the preventive interventions with the highest outcome impact per resource deployed.
AI in remote patient monitoring: care that doesn’t stop at discharge
AI in remote patient monitoring (RPM) extends clinical decision support beyond the hospital, enabling continuous observation and early intervention for patients managing chronic conditions or recovering at home.
The global AI in RPM market was valued at approximately $2 billion in 2024 and is projected to reach $13 billion by 2032 at a compound annual growth rate (CAGR) of 27.13%. That growth reflects a clinical reality: discharge does not end patient risk. Heart failure, diabetes, chronic obstructive pulmonary disease (COPD), and post-surgical recovery all generate clinically significant warning signals at home.
AI-powered RPM contributes to decision making in 3 distinct ways:
- Trend detection over noise. ML models process continuous biometric data from wearables and home devices, detecting trends rather than reacting to isolated readings. A single elevated heart rate is noise; a progressive upward trend over 36 hours in a heart failure patient is a signal worth acting on.
- Risk-based prioritisation. Predictive algorithms stratify patients by deterioration risk, so remote care teams direct outreach where it matters most rather than monitoring everyone with equal intensity.
- Workflow-native alerts. Signals surface within the clinician’s existing EHR or as structured triage summaries, keeping information actionable rather than buried in a separate dashboard.
By 2026, the U.S. Centres for Medicare and Medicaid Services (CMS) will release updated reimbursement codes expanding clinical applicability across both RPM and remote therapeutic monitoring (RTM), a regulatory signal that AI-assisted remote care is moving from innovation to standard infrastructure.
Generative AI in healthcare: giving clinicians their time back
Generative AI (gen AI) in healthcare reduces the administrative load on clinicians by automating documentation, note generation, and care coordination, freeing clinical professionals to focus on direct patient interaction.
A multicentre study of 263 physicians across 6 health systems found that clinician burnout dropped from 51.9% to 38.8% after 30 days of using an ambient AI scribe: a 25% relative reduction. That matters because cognitive fatigue is a direct driver of clinical errors, and any tool that reduces it has a downstream effect on care quality.
Ambient AI scribes capture clinical encounters passively, transcribe and structure the interaction, and populate the EHR note in near real time. The clinician reviews and approves rather than builds the record from scratch. The time saved, commonly 1 to 2 hours per shift, transfers directly to patient-facing time.
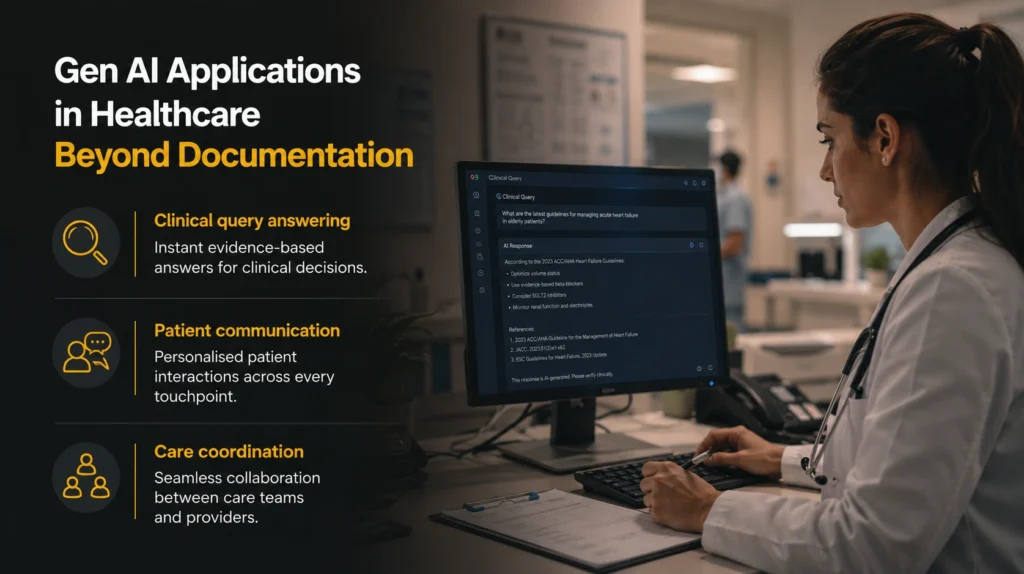
Beyond documentation, gen AI is being applied across:
- Clinical query answering. AI systems trained on guidelines and literature synthesise treatment options and case histories in seconds, compressing what once took hours of literature review.
- Patient communication. Gen AI drafts letters, discharge summaries, and follow-up instructions in plain language, reducing the administrative backlog after each encounter.
- Care coordination. AI flags gaps in follow-up, medication adherence, or pending referrals, ensuring nothing falls through the cracks between appointments.
The real challenges in AI decision making in healthcare
The primary barriers to effective AI in healthcare are not model accuracy. They are the structural problems of explainability, bias, integration, and governance.
Explainability. Many high-performing AI models operate as “black boxes”: accurate outputs, but no visible reasoning. A 2025 meta-analysis of explainable AI (XAI) in CDSS found that even where XAI techniques exist, they frequently fail real-world clinician needs for usability and workflow integration. A risk score that cannot be explained cannot be questioned; in a clinical setting, that is a governance problem as much as a technical one.
Bias. AI models learn from historical data, and historical clinical datasets frequently under-represent specific demographic groups, non-Western disease presentations, and patients with multiple co-morbidities. The same meta-analysis found that fewer than 15% of clinical AI papers included formal fairness or bias mitigation strategies. A model trained on biased data reproduces that bias at scale, and the populations most likely to be under-represented are often those with the greatest unmet clinical need.
EHR integration. Most health systems run on legacy infrastructure not designed to receive AI outputs in a workflow-native way. Retro-fitting AI CDSS onto existing systems requires significant technical effort. If the interface is poorly designed, alert fatigue follows: clinicians receive so many notifications that all of them, including critical ones, are eventually ignored.
Regulation. The EU’s (European Union’s) AI Act, which entered into force in August 2024, classifies most medical AI as high-risk. Requirements including formal risk management, data quality documentation, human oversight, and post-market monitoring become enforceable by August 2026. Organisations building or procuring clinical AI need governance frameworks in place ahead of that deadline, not in response to it.
What responsible AI clinical decision support looks like in practice
Responsible AI clinical decision support combines high-performing models with transparent reasoning, genuine workflow integration, and a human-in-the-loop design philosophy that keeps the clinician as the final decision-maker.
At Spark Eighteen, we built a clinical decision support interface for a digital health platform serving specialist care teams. The challenge was not model accuracy; it was adoption. Clinicians would only engage with a recommendation they could interrogate. The solution was to design the interface so every AI-generated alert surfaced the 3 to 5 signals driving it, the confidence level, and a direct link to the underlying patient data. Grounding the output in auditable evidence the clinician could evaluate and override materially improved both adoption and decision quality.
The principles that govern responsible deployment:

- Structural human oversight. AI-generated recommendations should require a deliberate clinician action to be enacted, not auto-apply without review.
- Population-specific validation. Models must be validated on the patient population they will serve, not assumed to generalise from a reference dataset built in a different demographic context.
- Continuous performance monitoring. Model drift, where accuracy degrades as real-world data distributions shift, is a genuine risk in clinical environments and must be tracked actively.
- Clear accountability from day one. When an AI-assisted decision contributes to a poor outcome, the clinical and organisational responsibility chain must be defined and known by all stakeholders before deployment begins.
These are not arguments against building clinical AI. They are the conditions under which it works.
The standard worth building to
The deeper promise of AI-based clinical decision support is not that it makes doctors faster. It is that it reduces the dependence of care quality on any single clinician’s availability, recollection, or current cognitive state. The doctor at the end of a 12-hour shift, the GP in a rural clinic without specialist access, the physician facing a presentation they have rarely encountered before: these are the people, and the patients behind them, who have the most to gain from AI that is built and deployed properly.
The measure of success is not the sophistication of the algorithm. It is whether a clinician in any of those situations makes a better decision for their patient than they would have made without it. That is the standard worth building to.
If you are designing or procuring a clinical decision support system and want to think through the architecture from both a product and data standpoint, reach out at coffee@sparkeighteen.com.